Short answer – Sehat Sahulat could help us get there, but there is a long way to go.
Pakistan has the highest neonatal mortality in the world, along with highest maternal mortality and the lowest life expectancy in the region as described by Macro Pakistani before. It is of course no coincidence that Pakistan is also one of the lowest spenders on health in the region, spending a mere 5% of general government expenditure on healthcare compared to Thailand which spends 15% of GGE on health or neighboring Iran which spends 22%. The low public investment in health means that people are privately spending out-of-pocket (OOP) with OOP spending making up 60% of Pakistan’s current health expenditure.
Universal Healthcare (UHC)
So how is this linked to UHC? UHC means that all people have access to health services they need, when and where they need them, without financial hardship. High OOP payments can lead to financial hardship in the form of catastrophic health expenditures, or impoverishment due to health expenditures. As the charts below shows, approximately 9% of all households in Pakistan face catastrophic health expenditures (10% of all expenditures) and 0.5% have been driven below the poverty line as a result of health expenses. This may seem small, but it does account for 20% of all households living below the poverty line. For very poor families, the high OOP can also act as a deterrent for seeking health care.
Households facing catastrophic health expenses by province and sector of care (% of total)
9% of all households in Pakistan face catastrophic health expenditures, mostly due to outpatient expenditures
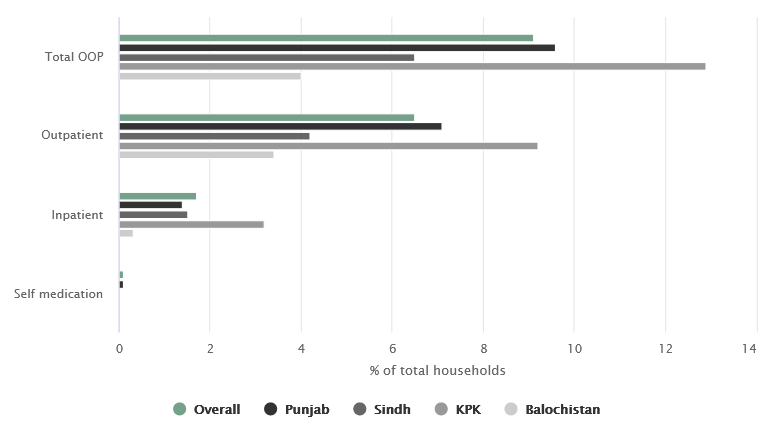
Source: PSLM 2018-19
Households driven to poverty due to health expenses by province and sector of care (% of total)
0.5% of all households in Pakistan driven to poverty due to health expenses (20% of all households)
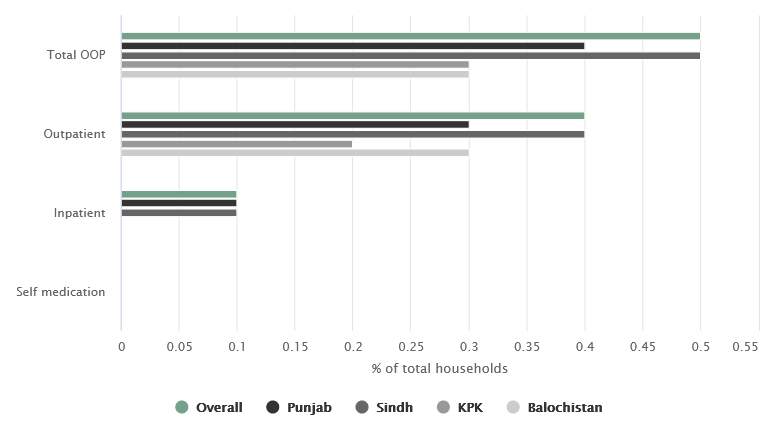
Note: Using $1.9 per capita per day as poverty threshold
Source: PSLM 2018-19
Sehat Sahulat, Pakistan’s novel social protection scheme can assist families in accessing care without incurring financial risk, but in order to understand the extent that it can support progress towards UHC, it is important to first start with what the program includes.
What is Sehat Sahulat?
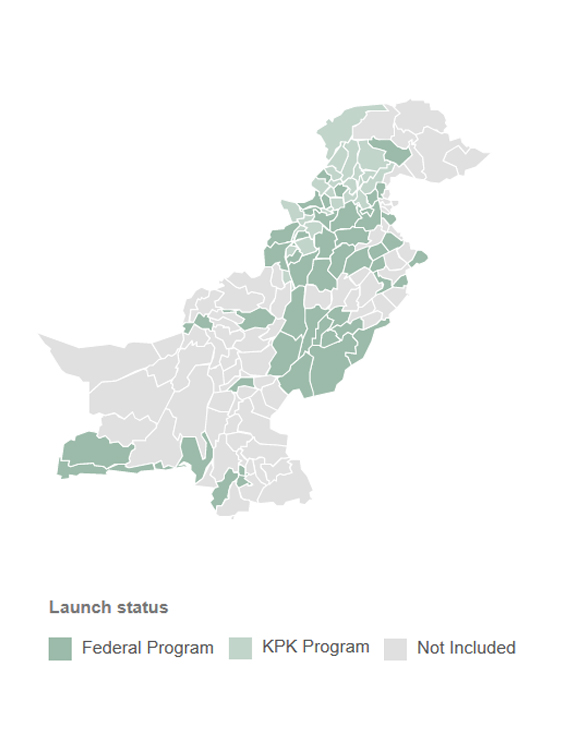
Source: PM Health Program
There are currently two separate programs called Sehat Sahulat, a federal program and a provincial program run by the government of KP. The federal program was launched in 2015 as the ‘Prime Minister Health Insurance Program’ by the PML-N government, but was then renamed to Sehat Sahulat in 2018. The provincial program called Sehat Sahulat was launched as a pilot in 2015 by the development firm GIZ and adopted by the provincial government of KP in 2016. The two programs provide coverage for inpatient services for a list of seven priority diseases at the provincial level, and eight priority diseases at the federal level (which also covers neurosurgical procedure). Initially both programs were targeted towards beneficiaries living below the poverty line, but the KP program is expanding to the entire population, and the federal program has expanded to include persons with disabilities and the transgender population.
The other main difference between the provincial and federal programs is that the provincial program provides coverage up to PKR 400,000 for tertiary hospitals, and PKR 40,000 for secondary care hospitals while the federal program provides coverage up to PKR 600,000 for tertiary hospitals and up to PKR 120,000 for secondary care hospitals. The Prime Minister of Pakistan has lauded these programs as important step towards building a welfare state. They are indeed remarkable and innovative initiatives pushing healthcare delivery in the right direction, but further expansion or support from the public health infrastructure may be required to achieve universal healthcare. Some of the major strengths and limitations have been described below.
Strengths of Sehat Sahulat
The program prioritizes the vulnerable: The initial beneficiaries of both programs included households living below the poverty line, who would find it most difficult to pay for inpatient treatment. The provincial program will be provided to all citizens early next year, but the federal program still includes the extremely poor, while also expanding to the transgender population and persons with disabilities. This outright mechanism of defining and explicitly prioritizing the poor and vulnerable is an excellent method of providing direct benefits to households that probably need it most.
The program effectively leverages the private sector: Different studies show that private sector utilization can be as high as 80% in Pakistan. Estimates from the national health accounts shown below shows that over 80% of all health expenditure occurs in the private sector. This program provides an effective way for governments to leverage the existing infrastructure of private sector facilities, while also ensuring that beneficiaries are not paying out-of-pocket. This approach to UHC is also in line with global findings, which recommend that private sector engagement and partnerships are critical to helping low middle-income countries (LMICs) in achieving UHC.
Usage of providers by public/private and type of care (%)
Private sector utilization of healthcare providers is as high as 80% in Punjab and Sindh
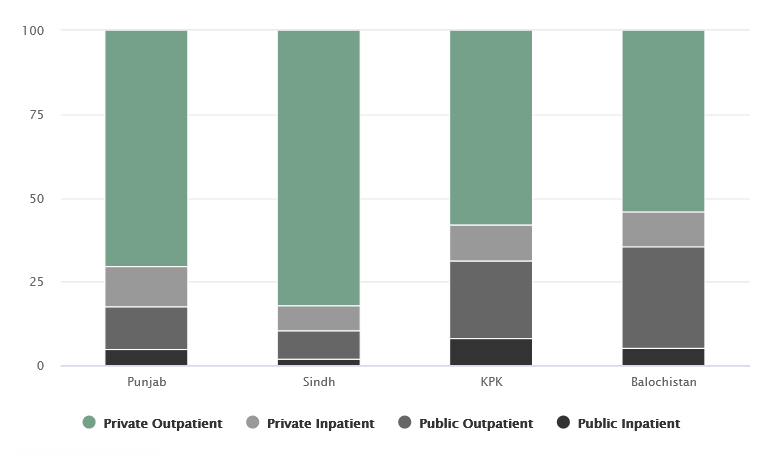
Source: An empirical analysis of OOP Health Expenditure Survey (Faraz Khalid, Wajeeha Raza, David R. Hotchkiss et al.), Household Integrated Economic Survey 2013-14
Sehat Sahulat covers high-cost treatments, and maternity care: The list of priority diseases includes treatments like cancer and renal dialysis, which are some of the highest cost treatments around the world that have shown to lead to impoverishment and catastrophic health expenditures. Populations living below poverty would have most likely forgone care for these illnesses due to a lack of affordability without the program. Sehat Sahulat also covers maternity care, which is important for reducing maternal mortality and increasing skilled birth deliveries, and also because it is the category with the highest average expenditure.
Opportunities for Sehat Sahulat
As mentioned above, Sehat Sahulat (both federal and provincial) are truly remarkable programs that are helping provide social protection to the poor and vulnerable. However, the current design of the program may not be sufficient to help Pakistan achieve UHC.
The entitlement is predominantly inpatient care: The benefits from the program mostly includes inpatient procedures requiring surgical care and emergency care treatments. The main exceptions include antenatal care visits, and follow-up outpatient visits following admission. The charts included earlier also show more than 80% of health facility utilization is for outpatient (OPD) visits, while 20% were for inpatient or emergency care. OPD visits are regular visits to the hospital for illnesses that are not emergency care and do not require hospital admission. Some examples of diseases that require OPD visits includes lower respiratory infections, mental health, dental care and hypertension (high blood pressure). These illnesses have high disease burdens, high cost and in some cases lifelong medication needs. OPD visits are also the biggest contributors to both impoverishment and catastrophic health expenditures across all provinces.
At the federal level, many ‘poor’ families are missed out: The current beneficiaries of the federal program includes populations living under the extreme poverty threshold of a household income of $1.9 a day, as well as transgender persons and persons with disabilities. According to the latest Pakistan Social & Living Standards Measurements survey, the population living below the poverty line is only 3.2% of Pakistan’s population. The survey also shows that over 20% of Pakistan’s population lives under the revised poverty threshold of $3.2 a day. This means that over 18% of households in Pakistan are poor by the World Bank classification but will not be eligible for the program under the federal program. UHC means that all people have access to the health services they need, when and where they need them, without financial hardship.If the federal Sehat Sahulat is expanded to the whole country, only 3.2% of population would be covered for inpatient care than before.
How to Save More Lives?
The current benefit package may not save the most lives. The “benefit package” for Sehat Sahulat refers to the diseases that are covered under the program. Typically what is covered in a national insurance program, or public sector provision is based on local evidence about the treatments that are found to be cost-effective. Treatments that are more cost-effective help save more disability-adjusted life years. All governments face constrained budgets, so if the government needs to decide whether it should fund chemotherapy or an angioplasty for instance, the more cost-effective treatment will allow the government to save the most disability-adjusted life years. This allows the government to gain ‘the most bang (in this case, health) for their buck’
Over the last two decades, global partners including the World Bank, the University of Washington and the Gates Foundation have been compiling evidence on cost-effective health interventions for LMICs called the ‘Disease Control Priorities’(DCP). In their latest update, DCP included a list of 219 interventions shown to be cost-effective across LMICs. This list does not indicate that renal dialysis or treatment for all forms of cancer are cost-effective. The government may be able to gain better population health or save more lives by investing in other services such as OPD care or preventative health for the same amount of money.
It is worth noting that there is currently an on-going national activity to contextualize recommendations from DCP to local evidence and define the most appropriate benefit package by the Ministry of National Health Services, Research and Coordination. In the future, perhaps this evidence can be used to redefine the benefits for the package.

